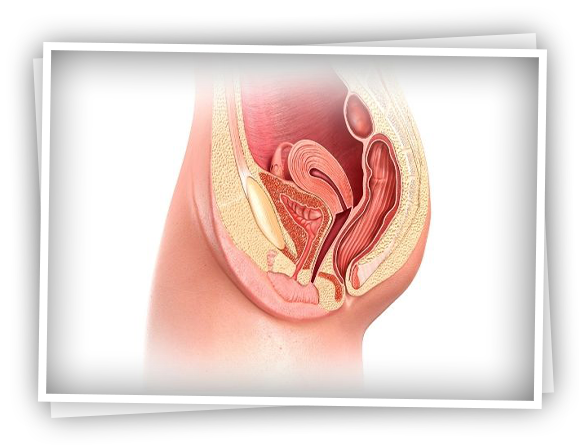
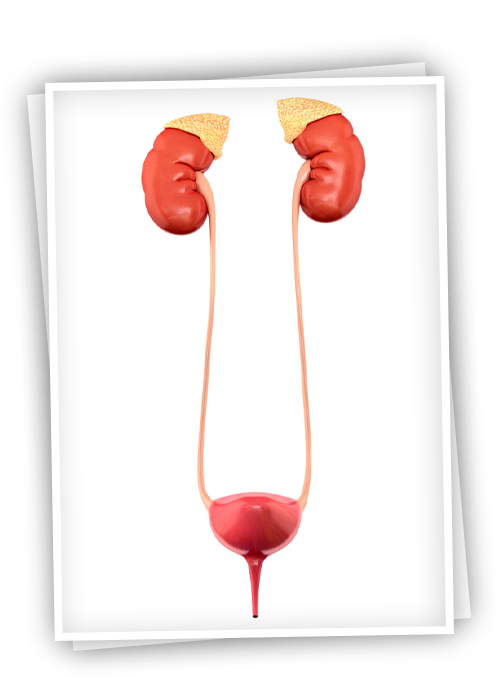
In patients with urethral stenosis, there is a problem in urination and the accumulation of urine in the bladder increases. Urine flow is severely troubled. They go to the toilet frequently, but the urine empties very thinly and slowly. There is no complete emptying and urine remains in the bladder each time. Apart from this, discharge problems occur due to thickening of the urinary bladder, and the urine accumulated in the bladder may disrupt the discharge of the kidneys. Urine accumulation leads to serious problems such as kidney infections and kidney failure.
In the presence of urethral stricture, the following symptoms are observed in the patient:
- Very thin and dripping urination
- Frequent urination
- Incomplete emptying of urine and constant feeling of fullness
- Bifurcation of urine
- Burning and pain on urination
Impaired bladder emptying does not allow any more urine to accumulate in the bladder, but the kidneys continue to produce urine. With the progression of the disease, the urine produced in the kidneys becomes unable to fill the bladder and begins to accumulate in the ureters. In the advanced stage, the kidney pools enlarge and kidney damage occurs. Inadequate drainage of urine may also cause cystitis-like urinary tract infections and serious complications related to them.
The patient's complaints primarily suspect urethral stricture. With the voiding test called uroflowmetry, it is determined that there is a weakening in the urine flow. The stenosis in the urethra and the location-level of the stenosis are determined by film (urethrography). In this film, a special liquid substance is injected into the outer urinary hole and the passage of the liquid is observed with x-ray. In addition, diagnosis and treatment can be done in the same session with urinary tract endoscopy.
There are basically 3 treatment methods. Expansion of the stenosis area, that is, dilatation, opening the stenosis area by cutting (endoscopic treatment-urethrotomy intern) and open surgery. Open surgery is applied to patients with long narrow segments who do not benefit from other treatment methods. With open surgery, the narrow part is removed and replaced with new tissue.
In the treatment of urethral stricture, first of all, detailed diagnostic methods should be applied. The patient's history and physical examination are effective in the diagnosis phase, but in addition to these, various radiological and endoscopic examinations may be required. Endoscopic examinations are among the most commonly used diagnostic methods. Thanks to these examinations, the stenosis in the urethra and related factors can be determined clearly.
With a film called urethrography, radiographic contrast material is given through the urethra hole to view the location and length of the stricture. In patients with a bladder catheter (cystofix), complete imaging is achieved by administering a contrast agent from this catheter.
In some patients, a procedure called cystoscopy can be performed to evaluate the exact location and length of the stenosis, prostate enlargement, bladder neck height, and bladder in detail.
Then, appropriate treatment methods can be started for the patient. In patients with severe obstruction, the priority is to provide relief by emptying the patient's bladder. For this, methods such as urinary catheter or catheter can be preferred. Or, in patients who cannot insert a catheter, a catheter is inserted into the bladder under the umbilicus (percutaneous cystostomistofix).
After the patient is relieved, surgical intervention is essential to eliminate the existing stenosis problem. In the endoscopic surgical procedure known as urethrotomy, it is aimed to widen the narrow urethra. In cases where urethrotomy is not suitable or successful, an open surgery method known as urethroplasty is applied. In this surgery, the most appropriate treatment method is applied to the narrow area of the urethra.
Surgical experience and the physician's command of different treatment methods are important in the treatment of urethral stricture. Each unsuccessful surgery may adversely affect the success of the subsequent surgical treatment. Therefore, such patients should be treated in appropriate centers.